Etiology: ACL tears are not the most frequent knee injury, but they are among the most serious. Return to play occurs usually around 6-9 months in a good outcome, and most say it takes 2 years to return to 100% (unless you’re Adrian Peterson). Approximately 200,000 ACL tears occur annually in the US alone, with an annual financial cost of almost 2 billion dollars. 70% of injuries are non-contact, and women have a higher incidence – reported from 2-10 x more than men, depending on the study and on the age of subjects. In general adolescent women had rates reported as high as 10:1 versus men, with among subjects in their late 20s women were about twice as likely to tear their ACL. This is likely attributable to participation changes in these demographics as we age.
OK this is a post which could get out of control long due to the multi-factorial nature of ACL injuries, so I’ll try to be concise. Here are a few of the primary risk factors for ACL tears:
Sport: Non-contact ACLs usually occur during landing or cutting, and usually during games (not practice/training). Therefore, sports such as football, basketball, lacrosse, and soccer among other cutting sports are high-risk sports for ACL tears.
Playing Surface: For field sports, there is a higher prevalence of tears on turf versus grass.
Previous ACL injury: Perhaps the largest correlation of a future ACL tear is the history of a tear. Compared to controls, there was a 10x greater probability of tearing either your graft or the contralateral ACL. This may be due to a number of factors including gender, the sport(s) you’re playing, congenital laxity, altered neuro-muscular performance, and more.
Ligamentous Laxity: generalized congenital laxity or acquired laxity (such as through knee hyperextension) both correlate to increased ACL risk. One thing I do try to emphasize to patients is the negative effects of knee hyperextension, as it compresses the fat pad and gives more laxity to the ligaments.
Q-angle: As talked about in the post on patellar dislocations , a higher Q-angle contributes to increased femoral medial rotation and knee valgus, both of which stress the ACL.
Altered NeuroMuscular Performance with jumping/landing/cutting:
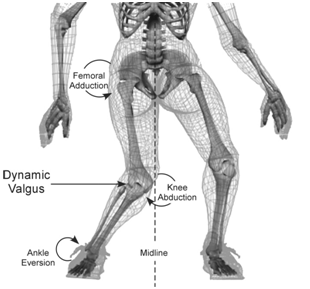
a. Eccentric hip abductor control: It’s shown consistently throughout literature that increased femoral medial rotation (found more commonly in women) correlates to increased knee valgus and more stress on the ACL. To me, the main problem is a imbalance between the Tensor Fascia Latae (TFL) and the posterior fibers of the gluteus medius and gluteus maximus muscles (aka your primary hip external rotators). If the person is unable to properly balance these muscles during eccentric activity (such as landing, cutting) increased stress on the ACL results.
b. lower abdominal strength: poor performance of the transverse abdominus and the external obliques results in increased pelvic and femoral rotation (medially) and therefore imparts more stress on the ACL.
c. altered hamstring vs. quadriceps timing during eccentric activities: Women have been shown to have decreased hamstring activation at initial contact (55% Max Voluntary Contraction vs. 72% in men). As the hamstrings are the secondary restraint (ACL is 1st) to anterior tibial translation, poor activation of them during sports may put undue stress on the ACL in an attempt to keep the tibia from translating forward.
Landing/Cutting on a straight knee: Landing on a straight knee is correlated to increased risk of ACL tear. Women have been shown to on average cut on a knee with decreased knee flexion in comparison to men. This is important as anterior translation of the tibia is far lower as the knee is flexed more during landing. It’s important for PTs to focus our effort in post-operative rehab or rehab for other knee pathologies to train these proper motor patterns into our patients.
Hormonal factors: During the mid-cycle time in a women’s period (the ovulatory phase) ligamentous laxity is increased and ACL injuries may be more common. Research by U of M’s Edward Wojtys in AJSM, March 2002, showed this and additionally that oral contraceptive use may have an element of a protective effect during this time period.
Conclusion: Contributing factors to ACL tears are multi-factorial. As a clinician, the most important factors we can control are the neuromuscular imbalances and altered form with landing and cutting. These may be the building blocks to ACL prevention programs which I will discuss in a future post.

Found your blog while browsing mgoblog one day and just wanted to say keep up the good work. As a UM alum, MGOBlogger, and a third year DPT student ready to take my boards, I couldn’t ask for a blog more tailored to my interests!